You reach a stage where filtration fails. Toxins build. Fluids overload. Blood pressure spikes. The nephrologist discusses options. Transplant waits elsewhere. Dialysis begins here. You’re asked to choose. Not between right or wrong—but between different kinds of artificial balance.
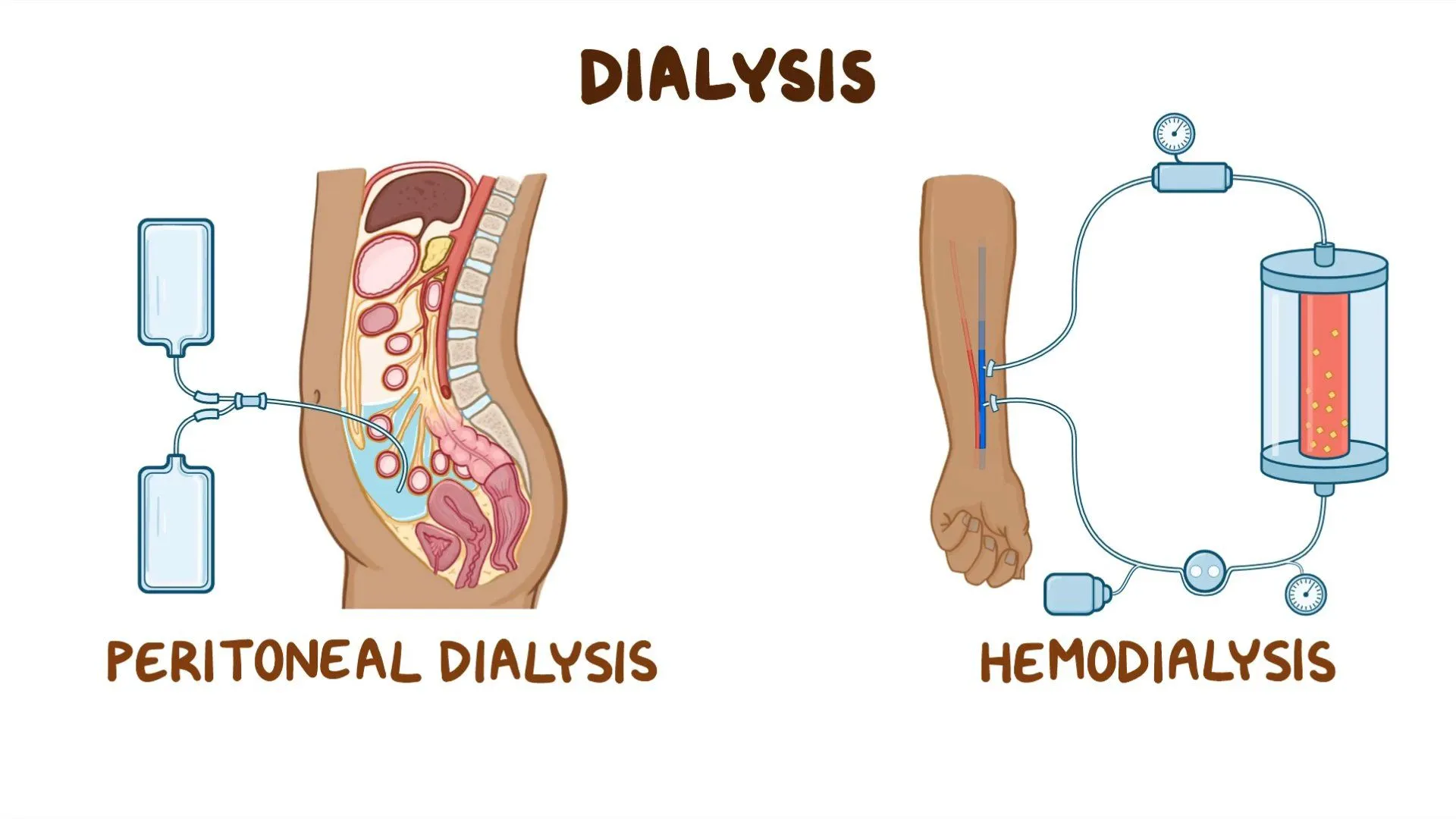
Hemodialysis uses a machine that filters blood through a dialyzer outside the body
A needle enters your arm. Blood exits, runs through tubing, enters the machine. It filters through a dialyzer. Toxins move out. Fluids shift. Electrolytes reset. Then it returns to your body. One circuit. Three to four hours. Multiple times per week. A rhythm begins.
Peritoneal dialysis uses the lining of your abdomen to filter blood from the inside
A catheter enters your belly. Dialysis fluid flows in. It sits. The peritoneum filters. Waste crosses from blood to fluid. After hours, the fluid drains. Another fill begins. No needles. No machines at the clinic. But more sessions per day. And more independence at home.
Hemodialysis usually happens in a center, under direct medical supervision and structured timing
You travel to a unit. Nurses guide you. Machines monitor vitals. Sessions follow a schedule. Monday, Wednesday, Friday. Or Tuesday, Thursday, Saturday. You lose flexibility. But gain oversight. Emergencies are handled fast. Stability is maintained. Predictability becomes part of the week.
Peritoneal dialysis often takes place at home, offering more control but demanding more responsibility
You do it yourself. Or a caregiver helps. Training happens first. Then supplies arrive. You manage timing. Cleanliness. Setup. Infection prevention. Some do exchanges during the day. Others use a cycler machine overnight. Freedom grows. So does personal accountability.
Hemodialysis moves fluid quickly, which can cause dizziness, cramps, or blood pressure swings
Fluid leaves fast. Blood pressure drops. You feel faint. Your legs cramp. Some need rest after sessions. The body reacts. Not every patient tolerates rapid shifts. Nurses adjust flow. But the speed can’t always be slowed. The machine dictates pace.
Peritoneal dialysis clears waste slowly, allowing gentler shifts but requiring daily consistency
There are no huge drops. No rapid pulls. But also, no days off. Every day counts. Each exchange matters. Skipping invites toxin buildup. Gentle doesn’t mean optional. Daily rhythm supports the system. Without consistency, clearance fades.
Hemodialysis requires access through a fistula, graft, or catheter in a central vein
Surgeons create a connection. Artery to vein. Over weeks, it matures. That’s the fistula. If veins aren’t strong, a graft goes in. Some start with a catheter. Each has risks. Each needs care. Infection, clotting, bleeding—all possible. But access is central to survival.
Peritoneal dialysis uses a permanent catheter placed in the abdominal wall under the skin
It enters low on your belly. Tunnelled beneath skin. Anchored in place. Exit site care becomes daily routine. Clean hands. Antiseptic. Dressing changes. It becomes part of your body image. Invisible under clothes—but always present during daily life.
Infections differ—hemodialysis risks bloodstream infections, while peritoneal dialysis risks peritonitis
Fever, chills, redness. Hemodialysis brings vascular risks. Bacteria enter the bloodstream fast. Peritoneal infections often begin with cloudy drainage, stomach pain. Different risks. Different responses. Both require vigilance. And both mean stopping if not caught early.
Diet restrictions vary—hemodialysis patients limit potassium, phosphorus, and fluids more tightly
You eat with caution. Bananas, oranges, tomatoes? Dangerous. Too much fluid? Swelling, shortness of breath. Hemodialysis clears waste less frequently. So everything accumulates between sessions. Your plate becomes math. Your cup becomes a scale.
Peritoneal dialysis offers more leniency with fluids and some dietary flexibility
More frequent exchanges mean less buildup. Potassium varies. Fluid intake loosens. You eat more freely. Still with guidance—but fewer bans. Diabetics adjust sugar intake carefully. Dialysate contains glucose. That affects blood levels. But overall, food becomes less strict.
Some patients switch methods when medical or lifestyle conditions shift over time
A hernia forms. The catheter clogs. Access fails. Blood vessels collapse. Or life changes. One method becomes harder. The other steps in. Switching isn’t failure. It’s flexibility. Treatment bends to fit the body’s story.
Both methods support life, but neither replaces what kidneys once managed continuously
You don’t get back what was lost. Dialysis sustains—not restores. It does the job in parts. Not every hour. Not every day. It mimics function. But never matches it. You adapt. You monitor. And you live with the compromise.
Fatigue remains common in both approaches, even when labs and schedules appear stable
You follow everything. But still feel tired. That’s expected. Dialysis doesn’t fix anemia fully. It doesn’t remove inflammation. It can’t reverse time. Energy dips. Mental fog lingers. Even good numbers don’t mean full vitality. Fatigue becomes the quiet partner in daily life.
Deciding between them means balancing freedom, oversight, effort, and tolerance for disruption
There’s no perfect method. Only the one that fits now. Some choose structure. Others want freedom. Some accept help. Others want solitude. The decision reflects body, schedule, emotion, support. You weigh trade-offs. Then move forward. With time, the decision often makes itself.
Source: Nephrology in Dubai / Nephrology in Abu Dhabi